
|
|
||
08/22/03 |
|
Pulmonary Arteriovenous Malformations (PAVM's)
What are PAVM's? They appear as 1 to 5 cm round, oval or lobulated masses, usually in the lower lobes of the lungs. They are present at birth and become apparent at different ages - normally in the 40's and 50's. PAVM's 'shunt' blood from the right (blue) heart system to the left heart (red) system without picking up oxygen in the lungs. This results in symptoms of low oxygen, shortness of breath and fatigue. In healthy individuals, de-oxygenated 'blue' blood returns to the heart and is pumped out through the pulmonary artery to the lungs. The blood passes through the capillaries on the surface of the lungs where oxygen is picked up. The newly oxygenated 'red' blood returns to the heart through the pulmonary vein and is then circulated around the body. PAVM's are direct artery to vein connections, with no intervening capillary network. PAVM's are generally of the fistula type, in other words high-flow low resistance lesions with a thin walled aneurysm (a sac-like widening of the blood vessel) between the feeding artery and draining vein. Another way of describing a PAVM is an abnormal communication between pulmonary arteries and pulmonary veins. It is a short circuit between the pulmonary artery and vein. Blue blood is fails to get to the capillaries on the surface of the lungs and is channeled back to the heart where it mixes with red oxygenated blood. The result is the overall concentration of oxygen in the 'red' blood is diluted with however much blue blood is bypassing the lungs through the PAVM's. It has been suggested PAVM's develop as a result of capillary development failure during fetal growth. Treatment The most practiced method for treating PAVM's is non-surgical. It involves closing down blood flow through the malformed vessel by a technique known as embolization. A heart catheterization is performed by passing a catheter through the heart into the feeding artery into the malformation. The malformation is then blocked (embolized) by use of a medical glue, metallic coils or small beads. The procedure should only result in a single night's stay in hospital for observation. The full shrinkage of the malformations may take 4 to 6 weeks. Surgery is an alternative, but the PAVM's will return if not completely removed. Complications PAVM's can lead to life threatening and debilitating complications. The most important complications are stroke, brain abscess, spontaneous haemothorax (bleeding into the body cavity) and massive haemoptysis (coughing up blood). Blood feeding through the very fine capillaries of the lung (~8µm diameter) acts as a very efficient filter of small blood clots and bacteria. It is believed that because PAVM's provide a direct connection through which these 'particles' can pass, the patient is more susceptible to stroke and brain abscess. Indeed patients with PAVM's need to take antibiotic medicines before dental work because of the potential for bacterial release into the blood stream that could get into the brain to form an abscess. Further, serious infections such as pneumonia are potential causes for brain abscess if not properly treated with antibiotics. The thin-walled aneurisms can be fragile leading to the possibility of bleeding if they rupture. The greatest risk from this particular complication appears to be in pregnancy. Children are at a relatively low risk. HHT (Hereditary Hemorrhagic Telangiectasis) It would be improper to finish this piece without mentioning HHT (also known as Osler-Weber-Rendu (OWR)). PAVM's are commonly associated with HHT. For more information on this condition, follow the link to the HHT page. Rebecca Rebecca appears to have many PAVM's distributed over most of her lungs. Her upper left lobe appears to be free of them (oxygen saturations measured at 94%), but the remaining three lobes have PAVM's. A heart catheterization procedure revealed that the worst affected lobe was her lower left. It seems coincidental that this is also where the pneumonia occurred. In this part of her lung, it is possible to identify about 30 separate PAVM's all less than a centimeter in diameter. The lower right lobe appears to have about 6 obvious PAVM's, slightly larger than those found on the left side. We are led to understand that there are one or two PAVM's in the remaining upper right lobe. The hospital embolized several PAVM's during a procedure that took place on 19th February, 2001.
Technical Explanation
The PAVM on the far left was giving the largest 'shunt'. You can tell by the size of the vessels entering and exiting the 'nodule'. This was the first PAVM that the Interventional Radiologist embolized.
Vessel 'A' is from the pulmonary artery (blue blood supplied from the heart). 'B' is the bulbous 'nodule. Vessel 'C' is the vein taking the blue blood back to the heart. What is significant about this picture is that the vessel in and, in particular, the vessel out are quite large in diameter. This means that there will be a lot of blood flow through this particular PAVM.
This is the same PAVM after embolization. The radiologist has inserted a platinum and Dacron fiber coil into the artery ('A' above) and this has caused the blood to embolize and block flow into the nodule ('B'). You can see that there is now no blood flow evident back to the heart through the vein ('C'). The nodule is still there, but in time it will shrink in size and die.
The coil is made up of platinum wire with fibers made of a synthetic material called Dacron. The coil is passed through the catheter to the required location, where it is released. In place in the blood vessel, it attempts to go back to it's original coiled shape, which accounts for the twisted shapes that it adopts in the radiographs. The small fibers of Dacron are incorporated to increase the thrombogenicity. Stainless steel versions were not used in this situation because they tend to be made to a thicker gauge and have a little too much tendency to spring back into the original coil shape with the risk of vessel damage. The pictures to the left show the coils in their fully wound conditions. They are supplied in diameters typically 0.010" and 0.016".
More Information Ontario Thoracic Review - Summer 2001 (Adobe Acrobat file) - Very good article
This site was last updated 05/04/02 |

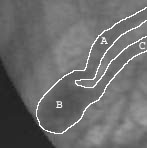 Here you can
see a close up of the PAVM with the large shunt.
Here you can
see a close up of the PAVM with the large shunt.
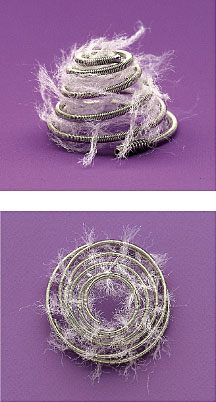 If you were to look at the coil under a magnifying glass,
you would see that it looks like a bottle brush with thin fibers extending
out along it's length. These help the embolization process as well as
giving some keying action with the blood vessel to hold it in place.
If you were to look at the coil under a magnifying glass,
you would see that it looks like a bottle brush with thin fibers extending
out along it's length. These help the embolization process as well as
giving some keying action with the blood vessel to hold it in place.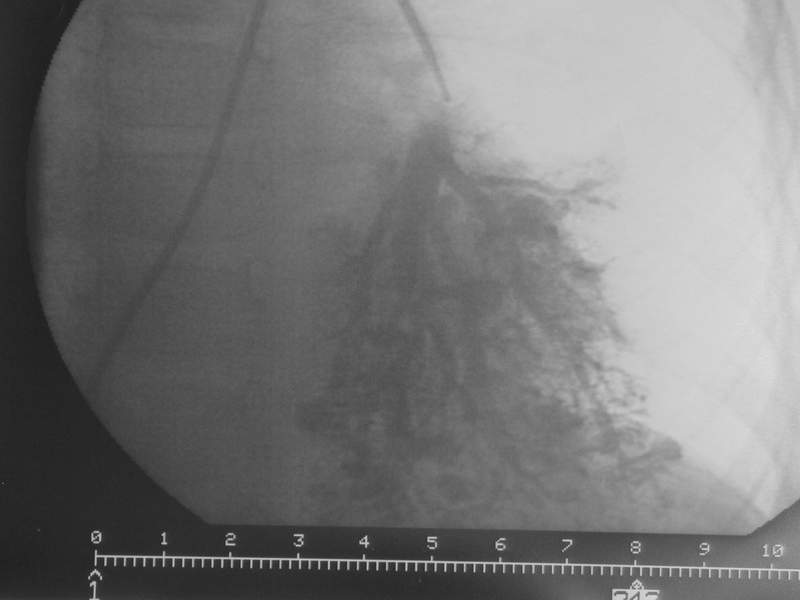{kind=link}
{kind=link}